
It is no secret that CMS intends to keep pushing the health care industry toward value-based reimbursement through its evolving payment models. The proposed rule for the Medicare Access and CHIP Reauthorization Act (MACRA) offers a new method of paying clinicians for the value of care they provide. It proposes implementing this change through a framework consisting of two paths: the Merit-based Incentive Payment System (MIPS) or advanced Alternative Payment Models (aAPMs).
However, CMS has made it clear that many of the current value-based models, e.g., Track 1 of the Medicare Shared Savings Program (MSSP), Bundled Payments for Care Improvement (BPCI) and Comprehensive Care for Joint Replacement (CJR) don’t involve enough risk to be considered aAPMs. This will likely force the overwhelming majority of organizations to comply with MIPS in very short order.
Meanwhile, the U.S. Department of Health and Human Services (HHS) and CMS have been hard at work creating new value-based programs eligible for aAPMs and releasing details on how CJR and BPCI programs could be modified to meet aAPM criteria. New programs include the Comprehensive Primary Care Plus (CPC+) program and a mandated bundled payment model for cardiac care, which sent shock waves through many organizations. Ultimately, as these models evolve and the health care industry continues its transition away from fee-for-service (FFS), designing the appropriate mix of methodologies and capitalizing on the success factors shared by each model will become essential to your value-based strategy.
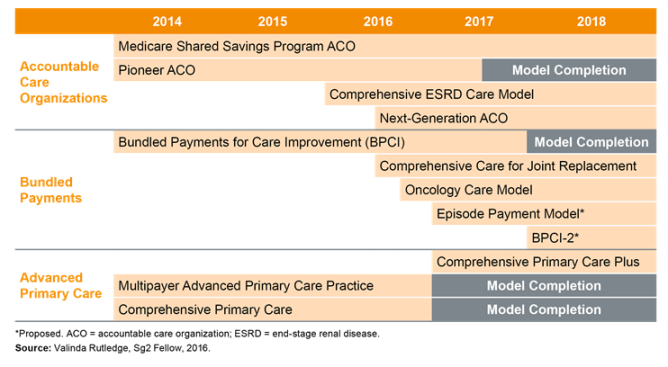
CMS Alternative Payment Models
Why are these models important and what do they mean for my organization?
Under the proposed rule for MACRA, clinicians who qualify for an aAPM are exempt from MIPS and qualify for a 5 percent incentive payment. The following models qualify for aAPM:
- MSSP: Tracks 2 and 3
- Next-generation ACO
- CPC+
- Oncology Care Model (OCM) with two-sided risk
- Comprehensive End-stage Renal Disease Care (CEC) Model
For those organizations looking to qualify for an aAPM, the deadline for application for MSSP Tracks 2 and 3 and for Next-generation ACO for 2017, have already passed. The 2-sided OCM model won’t be available until 2018. Clearly, this leaves limited options to qualify as an aAPM provider in the short-term, but understanding the models to chart a path over the longer-term is imperative.
Let’s take a closer look at the two new models as well as proposed changes in CJR and BPCI.
CPC+ is a multipayer advanced medical home model
CPC+ is designed around CMS’ previous pilot targeted at primary care practices. The model incentivizes changes in access and continuity of care; care management and coordination; patient and caregiver engagement; and planned care and population health. It is available in 14 defined regions through partnerships among CMS and commercial payers and/or state Medicaid agencies.
There are three elements of payment under CPC+: a care management fee paid per beneficiary per month, a performance-based incentive payment and FFS payments. These payment types vary across the two tracks of CPC+ that participants can choose from, with Track 2 involving risk and more opportunity for reward. Interestingly, CMS decided to allow a certain number of practices that are in MSSP to participate in CPC+, potentially providing an aAPM option for MSSP Track 1 participants who otherwise would not have had one.
Benefits of the CPC+ model include its multipayer design, which offers practices the opportunity to align incentives across participating payers (where payer participation is robust), which has been an ongoing challenge for many practices. It also appears to be relatively low risk. Additionally, payments under CPC+ come with some flexibility as to how they are spent, providing a revenue stream for investing in infrastructure as desired.
However, the CPC+ model still largely operates like a pay-for-performance program. Further, it does not incentivize primary care providers to reduce costs outside of the services provided by their practices. Lastly, CMS has not yet published the formula for how the prepaid and repayment amounts will be calculated, creating a challenge for practices wishing to fully assess this program before applying.
Organizations in the defined regions should assess whether or not CPC+ fits into their overarching strategy for value-based care. As applications for CPC+ are due September 15, 2016, interested organizations must move quickly, despite not having all the information they would like. CMS has more information about CPC+ and the application process.
CMS proposes mandatory bundles for certain cardiac and hip fracture care
My colleague, Chad Giese, recently covered the specifics of a new CMS proposal for a mandated bundled payment program for the treatment of coronary artery disease. It has been announced that there will be an aAPM option for this program, as well as for CJR, starting in 2018. At that time, different tracks will be introduced that would:
1) allow participants to bear risk for monetary losses that meets the proposed nominal risk criteria; 2) use quality measures that meet the proposed measure requirements to base payments; and 3) allow participants to opt into a track that requires use of certified electronic health record technology.
While the new cardiac bundles and CJR are mandated programs, CMS has also announced its intent to release a new voluntary bundled payment program (BPCI 2.0) in 2018, built on BPCI that could meet the criteria for aAPMs.
Assess your readiness for bundled payment participation
Whether mandatory or voluntary, Sg2 expects the rise of bundled payment programs to continue. We recommend that organizations assess their readiness for bundled payment from a cost, quality, partnership and physician alignment perspective; fully understand the programs and models that are available; and align care redesign for bundled payment programs with other value-based reimbursement programs that they currently participate in or plan to in the future.
Create your enterprise strategy for value-based payment
Clearly, CMS is taking steps to release additional models that allow both primary care physicians and specialists to qualify for aAPMs in the future. However, since there are limited aAPMs available for 2017, health systems should begin preparing for the impact of MIPS today. Simultaneously, they must chart their longer-term strategy for enterprise-wide value-based reimbursement and care delivery.
Keep in mind that this isn’t solely a choice between one model or another; it’s about offering the right mix of value-based methodologies across your organization. Not every model will or should be a fit for every organization, but understanding your organization’s short- and long-term goals, coupled with a detailed assessment of the new models and the other reimbursement changes within your market, will allow you to develop an enterprise-wide strategy for the transition to value-based payment and care delivery. Ultimately, health systems will need to determine which models should be a part of their risk portfolio, embracing the mandatory models and carefully selecting other models that advance system goals.

Sources: CMS. Comprehensive Primary Care Plus. CMS.gov. Updated August 29, 2016; Notice of proposed rulemaking for bundled payment models for high-quality, coordinated cardiac and hip fracture care. CMS.gov. July 26, 2016; Sg2 Analysis, 2016.