
"I want to see the best care available to all people. Just because you choose to live in a rural community doesn't mean you deserve less effective care." — Sherri Mason, Consulting Director, Vizient
By Erin Cristales, Vizient
Some of the first transcatheter aortic valve replacement (TAVR) procedures in the U.S. were performed in the Cleveland Clinic's Heart and Vascular Institute while Sherri Mason, now a Vizient consulting director, worked there as a clinical nurse. Throughout her career as a cardiovascular clinical trial manager and critical care registered nurse, she'd seen the brutal toll of heart disease and the long-term recovery required following open-heart surgery. The idea that TAVR could treat patients with no surgical options for their severe aortic disease — and one that, if proved successful, would offer a treatment that didn't require opening the chest — was astonishing.
"For a lot of patients, it's not just that they can't afford open-heart surgery — it's that they can't afford to leave work for the time required for full recovery following surgery," Mason said. "They may not have sufficient income, family support or benefits that allow them to recover for several weeks from open-heart surgery. But a TAVR allows them to, in many instances, walk out the door in one to three days."
Transcatheter aortic valve replacement is a minimally invasive procedure that replaces a diseased aortic valve with a tissue valve designed to be delivered into position via a catheter rather than an open-chest procedure. The procedure may be preferred in patients who have risk factors that can complicate open-heart surgery such as old age, previous heart surgery, history of stroke, chronic obstructive lung disease (COPD), liver or kidney disease, and diabetes. Aortic stenosis that goes untreated over time results in worsening heart failure and poor quality of life.
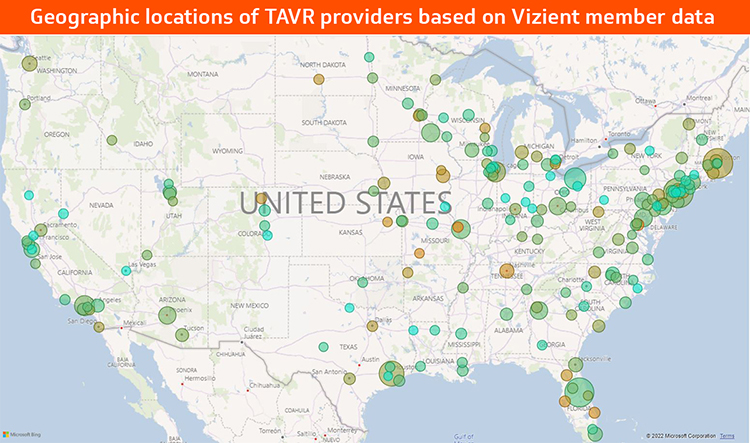
Of course, minimally invasive isn't the same as risk-free, and as the demand for TAVR increased — partly due to the expansion of availability to lower-risk and younger patients — Mason was curious to see how national industry data regarding the procedure compared to Vizient member data. She and Debbie Baker, Vizient consulting director for data applications and insights, found that in terms of length of stay, complication and readmission rates, the numbers largely aligned, as discussed in Vizient's recent Medical Device Tech Watch. But more revealing was a trend they noted: the clustering of clinics in several urban areas and an almost complete lack of access in many rural ones.
As it turns out, both are problematic. Clustering dilutes expertise, as TAVR procedures spread out among many doctors may make it more difficult to develop and maintain true proficiency. On the other hand, a paucity of clinics within an appropriate radius means many patients who could benefit from transcatheter aortic valve replacement may find it difficult or prohibitive to invest the travel time or expenses required to obtain treatment. Since a requirement for performing TAVR procedures requires an open-heart program to be available as back-up support, this also means that there may be few options for surgical valve replacement.
"In many places, there may be 10 different doctors implanting 10 TAVR devices," Mason said. "Would it not be more beneficial to stand up a new program in a locale where the population is underserved? Now you're not only ensuring the expertise needed for high quality outcomes remains optimal, but you're also ensuring that the people who will benefit have adequate access."
And Mason knows exactly what lack of access to cardiac care looks like. As a civilian working at an Army hospital in rural North Carolina, she was responsible for critical care transfers within the Veterans Affairs system, and often had to send patients to clinics that were hours away or only had two bays in the ER. As an RN in Albuquerque, she saw patients who had to routinely travel hundreds of miles to receive specialized care. Such medical deserts exist across the U.S., Mason says. West Virginia. Alabama. Mississippi. Everywhere.
One thing she learned from that Army hospital is to always follow a complaint with a solution. But that's where it gets tricky. "As a young doctor, would you rather live in North Dakota or Miami?" she asks. And then there's the circular issue of rural communities not attracting the providers necessary to establish an open-heart program — and an open-heart program having to be in place to establish a TAVR program.
But it's a challenge that can potentially be met through provider and supplier collaboration. Mason noted that when medical suppliers and hospitals partner rather than just contract, it deepens the relationship and promotes consistent care delivery and access for patients.
Take, for example, the patient-centered program that sprung from a collaboration between Mpirik, Medtronic and St. Francis Hospital in New York. Their partnership in the cardiac care pathway helped augment physicians' ability to identify, refer and treat patients, which led to interventions that may have otherwise been undetected. During a four-month period, 17 previously unidentified, undertreated patients were referred to a heart valve center — eight of whom received TAVRs. This evolving relationship addresses underserved populations and improves access to care.
What other types of strategies should be considered to help meet the needs of underserved communities? Finding ways to incentivize the right providers in the right locations, for one. There also are possibilities in perfecting the AI innovations that are rapidly revolutionizing healthcare, such as remote robotic procedures.
Equitable access to TAVR may be a puzzle, but it's one that needs piecing together. Just look at the data, Mason said. True health equity means ensuring patients can receive the treatments they need to save both their lives and livelihoods — no matter where they live.
"I want to see the best care available to all people," Mason said. "Just because you choose to live in a rural community doesn't mean you deserve less effective care."