
As we gear up for a busy autumn, CMS’s recent release of claims data related to the Bundled Payments for Care Improvement Advanced (BPCI-Advanced) program has increased anxiety among providers across the country. Those participating in, or considering entering into the program for Model Year 3 face the daunting task of culling three years of claims data and target-pricing sheets encompassing both peer and risk adjustment factors in search of opportunities to reduce Medicare spend for acute hospitalization plus 90 days post discharge care.
The BPCI-Advanced program is classified as a voluntary alternative payment model. CMS provides claims data to help participants determine which eligible clinical episodes, such as cardiac arrhythmia or hip and femur procedures, they wish to enter into. That decision is critical because BPCI-Advanced is a risk-based program inclusive of both upside and downside risk. Episode selection significantly influences financial performance and means the difference between receiving a positive NPRA (net payment reconciliation amount) from Medicare and writing a check to CMS to cover spend above the target price. Hence, careful and informed analysis of these data is essential for a participant’s decision to enter the program.
Data analysis is also vital to whether the participant is “going it alone” or is “under the wing” of a convener, a participant who facilitates and coordinates downstream entities known as episode initiators, which must be acute care hospitals or physician group practices. When working with a convener, hospitals and physicians should have an unbiased eye toward episode selection. Such objectivity enables meaningful, informed discussions with the convener, who may recommend an episode that makes the hospital or physicians uneasy for quantitative or qualitative reasons.
One other important consideration: the extremely short time frame between the receipt of data and the episode selection deadline. CMS’ BPCI-A Model Team has established Dec. 1. as the deadline for clinical episode selections and participation terms. Providers must be prepared to complete their build-out of the data files in short order to ensure ample time for discourse among all parties. Sg2’s recommended approach to data analysis entails starting at a macro level for each episode by breaking down Medicare spend in each area and comparing to benchmarks for best practices.
Avoid Analysis Paralysis by Following These Steps:
As many providers will attest, reducing spend in episodic models such as BPCI-Advanced starts by focusing on care coordination after the patient is discharged from the hospital. Therefore, prime episodes for consideration are those where at least 50% of the overall spend occurs outside the four walls of the hospital.
- Sg2 recommends filtering out episodes where the majority of spend is directly related to the MS-DRG (Medicare-Severity Diagnosis-Related Group) or procedure payment (for outpatient episodes)—a variable you can’t reduce.
- Next, align the remaining episodes around surgical/medical conditions or, if your organization is service line-centric, around specific service lines (e.g., cardiac, orthopedics, spine, general surgery). Then prioritize by volume e.g. 50-100 annual discharges.
- Finally, break down the episodes into concise buckets of spend (again, setting aside the MS-DRG payment) and utilization. Data analysis will highlight specific areas of opportunity—as well as risk—regarding key performance indicators, including the many post-acute spend buckets that CMS will be holding program participants accountable for.
For surgical cases, focus on key areas of care and spend, such as readmissions and causes, skilled nursing facility (SNF) utilization and length of stay, and use of inpatient rehab (see episode data sheet below for an example).
For chronic conditions, be certain to include emergency department use for follow-up care vs. alternative care settings, patient follow-up with the primary care providers or care managers within 24 hours to seven days of discharge, and social determinants of health relevant to patients and their families.
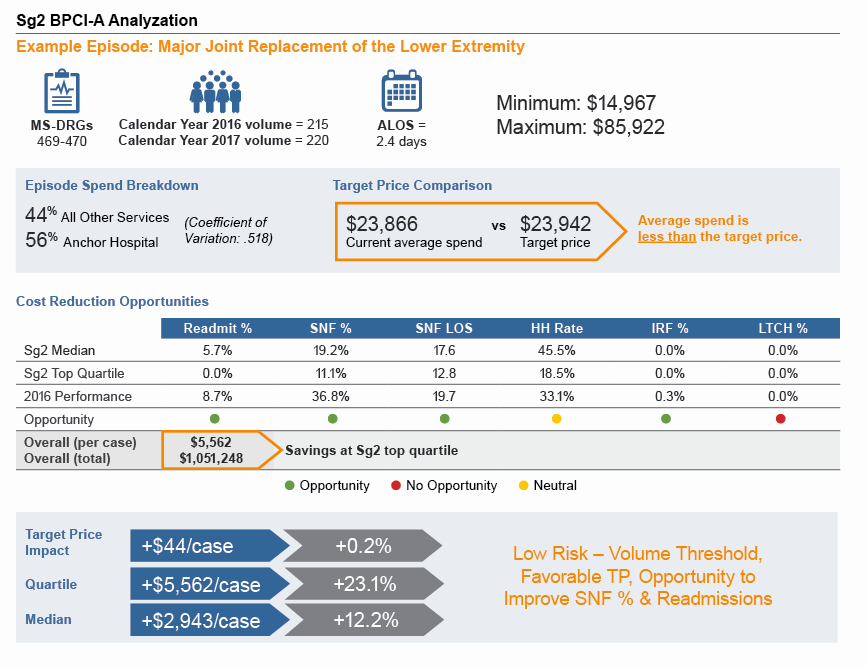
SNF = skilled nursing facility; HH = home health; IRF = inpatient rehabilitation facility; LTCH = long-term care hospital; TP = target price.
Time Is Not on Your Side
Participants have little time to comprehensively analyze the data and make decisions. Data must be downloaded, compiled and given to physicians and hospital leaders in a digestible format within days to enable as much time as possible for discourse. Opportunity for thorough deliberation allows the organization and physicians to commit to episodes for which risk has been carefully evaluated and the likelihood of success is high. This quantitative analysis must then be paired with the qualitative aspects of the program, including key components such as:
- Performance across the quality metrics
- Accountable care organization interaction
- Hospital-physician alignment
- Patient attribution across the market
- Value-based care infrastructure
Due to this complexity, a digestible set of data should be provided to leadership within 1-2 weeks from receipt.
If your organization is considering entering into BPCI-Advanced as a system, or minimally with multiple facilities as episode initiators, a careful evaluation of the data is essential to establish where common, effective approaches to reducing Medicare spend can be deployed, as well as where significant differences in care approaches exist across markets or the system. Moreover, the data provide insight into how various post-acute providers perform, thereby enabling the initial exploration of post-acute care networks to help ensure BPCI-Advanced success.
If you have any questions or need support for this extremely important process, please contact me or learnmore@sg2.com.
Additional BPCI-Advanced Resources
- Webinar (on-demand): Take Advantage of BPCI-A for Bundled Payment Success
- Blog Posts
