
by Kellie Goodson, MS, CPXP
Director, Performance Improvement Networks
As America begins to open back up for business, many of us are asking why now, what’s changed? We’ve been told for weeks, even months, to stay home. So what’s different? What makes it safe now? These sentiments not only apply to restaurants, retail shops, travel and tourism, but to health care as well.
Many health care organizations are making plans to reopen health care services, specifically by restarting elective procedures. Guidance from professional associations and industry experts about doing this safely is abundant, however, patients needing care may not behave the way we expect. In his article published in the New York Times last month, “Where Have All the Heart Attacks Gone?,” Dr. Harlan Krumholz contemplates the answer, including fear of going to the hospital and getting infected with coronavirus to changes in behavior patterns due to social distancing. Clearly, we can only speculate the additional reasons patients may be choosing to delay care.
When it comes to restarting elective procedures, health care organizations need more than speculation about how patients might behave – they need to be able to accurately forecast demand to ensure they have the proper capacity, supplies and staffing in place. The guidance provided by professional associates and industry experts is necessary, but leaves out a key piece of the puzzle: patient behavior.
Vizient, and our health care intelligence subsidiary Sg2, wanted to better understand patients’ thoughts about the reopening of health care services, specifically elective procedures, and how they will make decisions in the “new normal.” To gather this insight, we invited patient and family advisors (PFAs) to join us in a conversation via webinar earlier this month. As patients or family members of patients who have received care at a health care organization, PFAs partner with the provider organization to make improvements based on their experience. Health care administrators, clinicians and staff engage PFAs through Patient and Family Advisory Councils, where their feedback is leveraged in the strategic planning and operational improvement efforts of the organization.
We were joined by more than 40 PFAs from across the country who were not only geographically diverse, but had diverse backgrounds, experiences and roles (some patients, some family caregivers). You can read the summary report from the discussion for all the details, but what became clear was health care facilities must thoughtfully plan their reopening and communicate often with patients and families. The key will be to consider how patients may perceive their risks of exposure to COVID-19 versus the benefits of moving forward with their procedure as expressed in the figure below.
Figure 1. Person considering an elective procedure based on their perceived risk of exposure to COVID-19
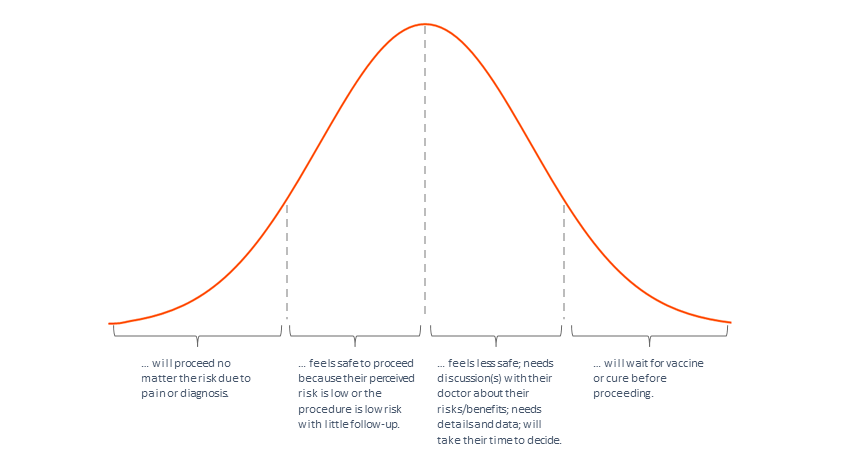
When these first two waves are scheduled for their elective procedures, physicians will need to engage the next potential group of patients¾those who feel less safe¾to ensure a steady stream of business. These patients will likely have many questions and will need to have discussions with their doctor about their risks and the benefits of the planned procedure. They will need details and they will need data. Details like the patient flow from pre-procedure through discharge with instructions and checklists to help patients and their family caregivers understand what will happen to keep them safe. Data such as the number of patients with COVID-19 currently in the facility, numbers of staff with active COVID-19 diagnosis and those who have recovered from it. Data can also include the number of elective procedures successfully completed so far and infection rates of patients who completed the same procedure. This third wave will take their time to decide. They want to know why hospitals and health care facilities are safe now, and no detail is too small to communicate to them.
Discussions and data won’t help the last group of patients move forward with elective procedures. They will wait until there is a vaccine or a proven cure and there will be no convincing them to do it sooner. Health care facilities must thoughtfully plan their reopening. A key component is how patients perceive their risk of exposure to COVID-19. Answering the questions of why now and what’s changed will help most patients make decisions about seeking care.
About the author
