
by Deborah Roy
Principal, Clinical Advisory Solutions
This blog post is part five of a five-part series on clinical-supply integration, a process for informed business decisions that engage clinicians, preserve quality and safety and lead to greater patient satisfaction. Read the other blogs in this series:
- Transitioning from Value Analysis to Clinical-Supply Integration: It’s All About the Process
- Getting from Good to Great: Using Data to Move From Traditional Product Standardization to Clinical-Supply Integration
- Moving from Value Analysis to a Clinical-Supply Integration Model: Engagement and Alignment are Key
- How Do You Know What You Know? 3 Ways Clinical-Supply Integration Can Help You Make Better Decisions
For years, health care supply chain professionals have been charged with balancing cost, quality and clinician preference when introducing new products and technologies to the organization. We often refer to this process as value analysis work and, more recently, it’s been referred to as clinical-supply integration.
Is there really a difference between the two concepts?
The short answer is yes. In this post, I’ll explain the difference to help you understand where you are on the journey toward achieving clinical-supply integration. We’ll also cover some of the industry changes that have prompted the shift.
The following graph shows the evolution from traditional value analysis to the advent of clinical-supply integration:
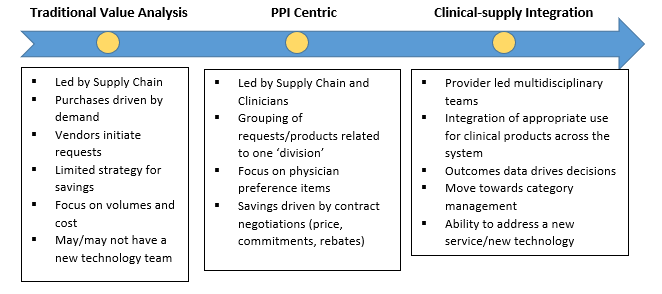
The Difference
Value Analysis
Value analysis is a method to respond to any new product requests across the organization. Over time, it has evolved to denote combining the right people, the right data and the right rigor to support product decision-making. The value analysis structure supporting product management can range from a loosely, ambiguous process to a consistent policy-driven practice.
Dedicated resources typically include supply chain staff and their analyst and, depending on the facility, a small group of engaged end-users that represent nursing staff and physicians. Data is focused on spend, volume and price. Occasionally more defined financial data and evidence is used, which can lead to a more informed decision. The executive team may oversee the process by providing guidance and savings targets.
Physician preference items
Moving along the spectrum, physician preference items have received greater emphasis in recent years due in part to a more defined focus on areas of highest expense, including the operating room and other procedural areas. Clinician end-users are brought into the product decision-making process for limited, targeted intervals. The clinician end-users review upcoming contracts, are privy to benchmarks, and often sit at the table during vendor negotiations. Standardization became a buzz word with goals to reduce market share for some product categories and increase for others.
Clinical-supply integration
Over time it became evident that clinicians expected more from their executive leaders. In turn, leaders now anticipate more from their clinicians. So, where is the happy medium? Clinical-supply Integration (CSI) offers the opportunity for collaboration while providing a process for informed business decisions that preserve quality, safety and patient satisfaction.
Advancing toward clinical supply integration
The first step is to commit to cultural change that engages and sets accountability at the clinical level, with support from the executive level. Make sure all parties understand what everyone’s roles are and how performance data will be reviewed and tracked. Most organizations at this juncture realize two things: high variation of products leads to overutilization and a lack of understanding of financial implications produces higher costs overall.
Clinicians are continually seeking actionable data about how their practice and utilization patterns affect overall procedure costs and outcomes. When providing data to your clinicians, consider the following:
- Be transparent with data, both in design methodology and comparison against peers or other organizations
- Ensure the output is consistent in presentation and availability
- Consider evidence, or lack thereof, when determining if a change in practice or product will improve outcomes
- Close the loop from initial identification, data development, negotiations, approvals, and conversion, and incorporate periodic non-biased audits to add credibility to the process.
Clinical-supply integration is a journey; over time, a sustainable process that works for an organization’s unique culture will become apparent. Components of the journey include engagement and alignment of the clinicians and the executive team with ancillary departments, including supply chain and value analysis teams.
Meeting agendas populated with requests will shift to agendas full of ideas that affect patient outcomes. Clinical peers will challenge each other to remove unnecessary variation, all supported by actionable, quantifiable and insightful operational and financial data. Clinical evidence, validated by the organization’s clinicians, provides the final set of information necessary for making informed product decisions. This process creates a virtuous circle that can become sustainable over time.
The logistics of moving toward clinical-supply integration takes a commitment from everyone involved. And, it’s a given that the process will need to flex and change over time. Being adaptable to how data is received, what software platforms are necessary and helpful, and who will maintain those tools is a learning experience.
Committee leadership will change. However, choosing leaders who can most effectively jump start your clinical-supply integration program is critical. Leaders need to know that one of their roles is to mentor the next leader for their position. The entire organization then will understand that they are all part of the process, cementing this vision and mission of the initiative.
The future of clinical-supply integration
What the future holds is uncertain. But knowing the rapid pace of change in health care, we need to be open to change and able to swiftly incorporate those changes into managing how we work with providers. One thing that is certain is our common goal is to deliver the best quality, safety and outcomes at the best value to patients.
With value-based care market demands increasing, thought must be given to measuring or quantifying quality. New payment models will require hospitals to provide better care with smarter spending. In the future, performance measurements could include improvement to health care processes, outcomes and patient experience. Did the selected product/procedure provide true value and enhance the quality of care?
Looking ahead, another change we may see is more patient involvement in product decisions, as patient satisfaction and experience continue to be at the forefront of hospital administrators’ minds. With the advent of patient and family councils, some councils are already involved in product discussions, such as providing feedback on implant satisfaction post-discharge.
The world of health care is ever-changing. As it evolves, we need to adapt and grow to find new ways for our clinicians to provide the highest value care and outcomes to our patients.
Clinical-supply integration is an ongoing, interdisciplinary strategy encompassing four performance domains — engagement, insights, process and knowledge — to inform decision making about products and services in order to eliminate harm, improve outcomes and lower costs. Read about the domains in the related articles below or learn more about clinical-supply integration.
About the author

With more than 30 years of experience in the health care industry, Deborah Roy has held numerous leadership roles responsible for the creation, development and measurement of value analysis teams, and clinical supply integration effort consistently exceeding targeted savings projections. In her role as principal at Vizient, Roy leads efforts to assist our members in achieving best practice protocols for how members can optimize clinical integration across all clinical operations. Partnering with organizations to apply accountable, provider-led decision-making principles, she creates governance processes that lead interdisciplinary teams in the development of customized approaches that support clinical and budgetary goals.